Recent searches
Search options
Administered by:

Here's a #physiology teaching case that *everyone* who touches a ventilator needs to understand:
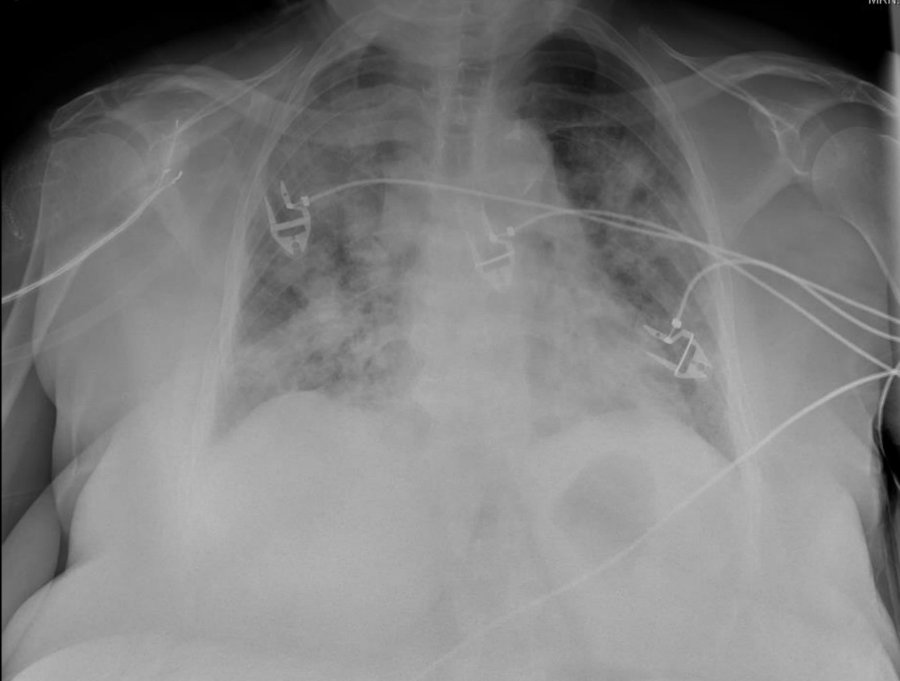
A 60 yo woman is intubated for hypoxemia from pneumonia. She has a SpO2 of 88% on PEEP +12 and 100% FiO2. PEEP is increased to +16 & her SpO2 drops to 80%.
What happened?
1/
1/
Let's start with a little multiple choice. Which mechanism(s) could contribute to hypoxemia in this patient?
2/
The answer is ALL of the above!
But why? To answer, we need to understand what PEEP is and what effects it has on the lung.
3/
Positive end expiratory pressure (PEEP) is the pressure above atmospheric that is applied in between breaths while on a mechanical ventilator.
PEEP is beneficial for two reasons: PEEP recruits collapsed lung (see video)
PEEP recruits collapsed lung (see video) greater alveolar pressure drives more O2 into the blood (Henry's law)
greater alveolar pressure drives more O2 into the blood (Henry's law)
4/
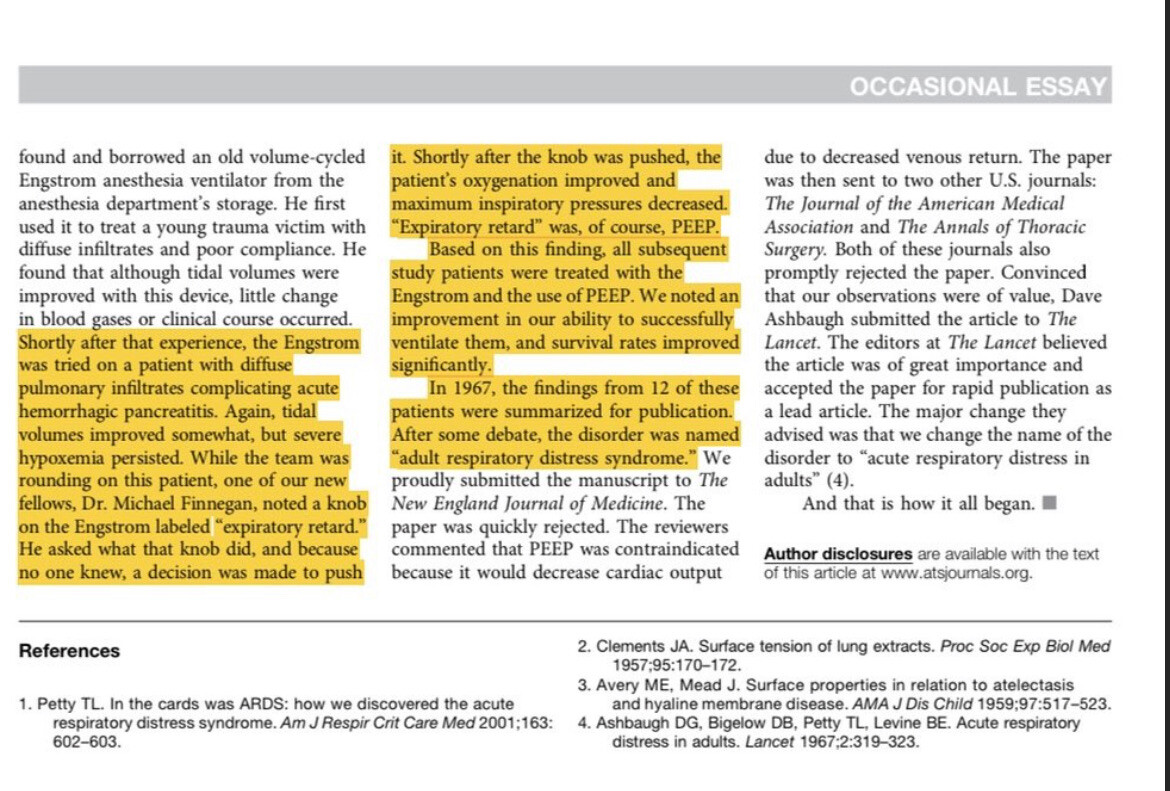
As an aside, it's worth noting that the benefits of PEEP in ARDS were discovered *accidentally*.
In 1967, two doctors caring for a patient on a ventilatory spotted a knob labeled "expiratory retard" and - not knowing what it did - decided to give it a try. It worked!
Nowadays we call that knob PEEP and it's an indispensable part of mechanical ventilation.
https://pubmed.ncbi.nlm.nih.gov/28731363/
5/

Ok so we understand why PEEP can help, but why can PEEP be *harmful*?
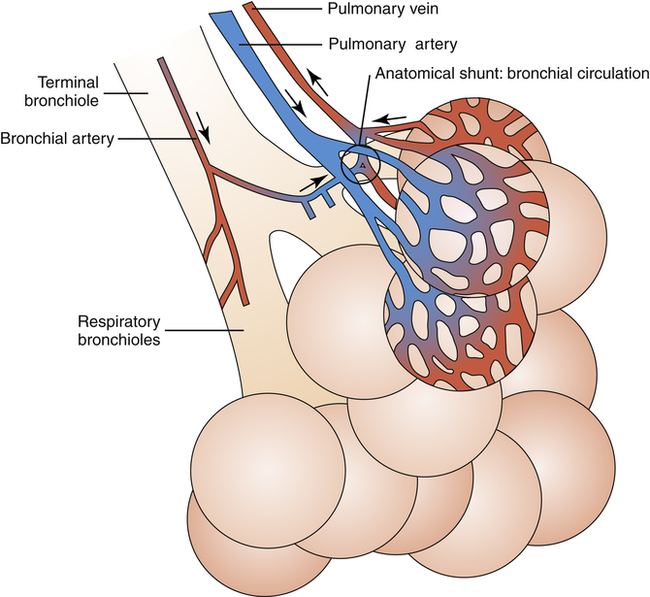
We need to understand the relationship between lung volumes & pulmonary blood flow.
Let's take a closer look at the alveoli. With the help of an electron microscope we can see that alveoli are surrounded by a dense interconnected network of blood vessels.
(btw, if you were wondering, they obtain these amazing images by injecting the vessels with a polymer, dissolving the remaining tissue, then taking SEM micrographs)
6/


@nick These images are taken with an SEM, not TEM. https://en.m.wikipedia.org/wiki/Scanning_electron_microscope
 @nick@med-mastodon.com
@nick@med-mastodon.com@MReyesM yes my bad. Typo